Could Cardiac Amyloidosis be a side effect of Covid-19 mRNA vaccination?
Here are some points to consider:
Cardiac Amyloidosis is listed in the Post Marketing Adverse Events of Special Interest in the Pfizer documents.
As of April 2023, a literature review, Leung W-Y et al, found three case reports that have concluded that Cardiac Amyloidosis was a side effect of mRNA vaccination.
There is a plausible aetiology according to Leung W-Y et al.
Since April of 2023 a far more plausible aetiology has come to light: mRNA frame-shifting, caused by the mRNA translation process skipping the fake methyl-pseudo-uridine.
Cardiac Amyloidosis
Cardiac Amyloidosis is a fairly rare disease, caused by a deposit of amyloid protein in the cardiac tissue and around the heart. Amyloid proteins are misfolded proteins; in order to be transported around the cell and through the body, proteins must fold correctly. If something goes wrong with the DNA or RNA transcription process, the cell may produce misfolded proteins.
FirstFactCheck is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
If such misfolded proteins, or Amyloids, build up in the brain, they can cause diseases such as Alzheimer’s disease or Creutzfeldt-Jakob disease. If they build up in the heart, they can prevent the heart muscle from being able to beat properly.
Pfizer Adverse Events
Cardiac Amyloidosis is listed in the Pfizer document, “5.3.6 CUMULATIVE ANALYSIS OF POST-AUTHORIZATION ADVERSE EVENT REPORTS OF PF-07302048 (BNT162B2) RECEIVED THROUGH 28-FEB-2021 - LIST OF ADVERSE EVENTS OF SPECIAL INTEREST” as one of the Cardiac side effects.
Some misinformation online has claimed these adverse events of special interest are just hypothetical or possible adverse events: they are not, they are real adverse events catalogued by Pfizer after the experimental mRNA vaccination had already been rolled out.
You can also look it up in my book, Transgenic, in which the Pfizer side effects are listed, ordered by medical category.
Literature Review
This is the literature review I mentioned at the start that looked at case reports in April 2023:
Leung, W.-Y.; Wu, H.H.L.; Floyd, L.; Ponnusamy, A.; Chinnadurai, R. COVID-19 Infection and Vaccination and Its Relation to Amyloidosis: What Do We Know Currently?Vaccines2023, 11, 1139. https://doi.org/10.3390/vaccines11071139 https://www.mdpi.com/2076-393X/11/7/1139#B64-vaccines-11-01139
Here is what Leung W-Y et al say about reported cases of Covid-19 vaccination induced amyloidosis; note that this is a Creative Commons 4.0 article so it is quite okay for me to quote this passage:
Reported Cases of COVID-19 Vaccination Induced Amyloidosis
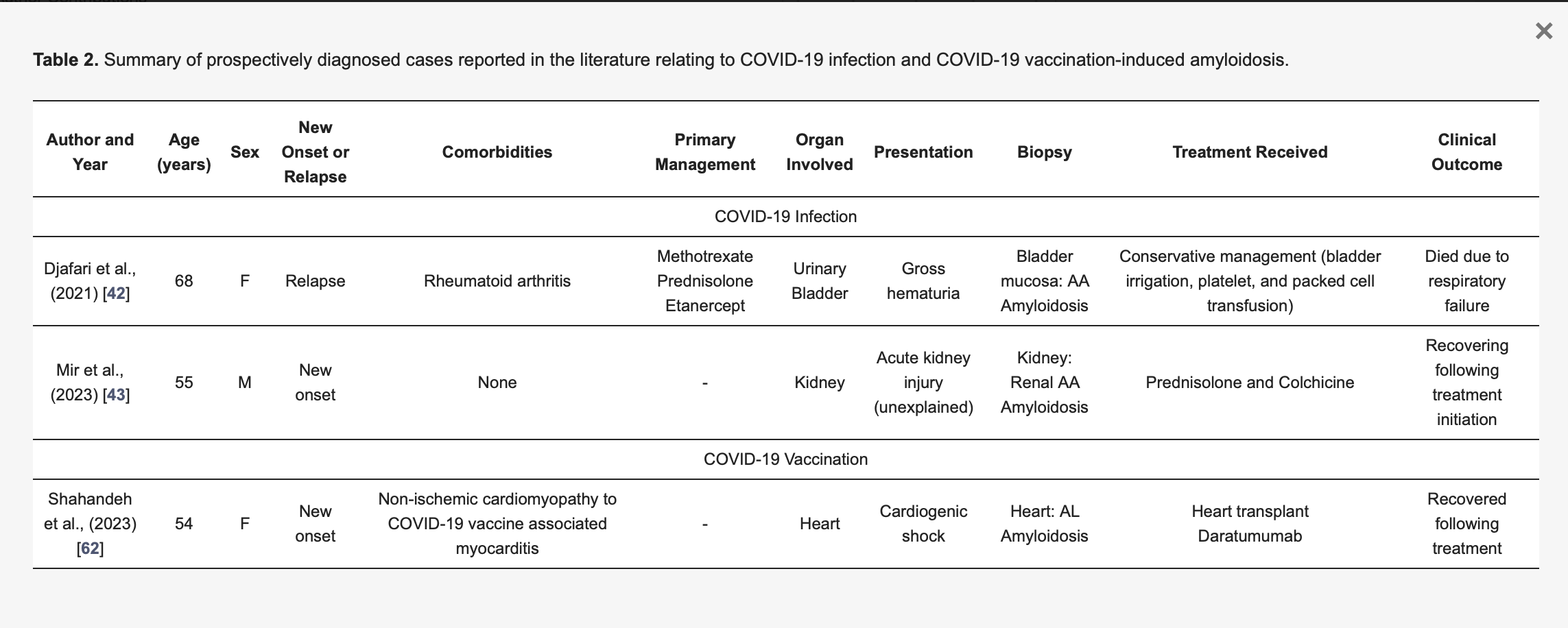
Table 2. Summary of prospectively diagnosed cases reported in the literature relating to COVID-19 infection and COVID-19 vaccination-induced amyloidosis.
The first case they looked at had myocarditis following vaccination. Her heart was in shock and they gave her a heart transplant — when they examined the heart that had been taken out, they found that the reason her heart was in shock was that she had Amyloidosis.
Shahandeh et al. [62] (see Table 2) reported a 54-year-old woman with a background of recent non-ischemic cardiomyopathy attributed to COVID-19 vaccination-induced myocarditis presenting with cardiogenic shock. She received mechanical circulatory support followed by uncomplicated heart transplantation. The explanted heart pathology confirmed a diagnosis of kappa AL amyloidosis. She was commenced on daratumumab monotherapy with no evidence of disease relapse on surveillance endomyocardial biopsies.
Leung W-Y’s assessment of the second — very horrifying — study appears to be biased: I think you should read the study for yourself. This poor guy, a previously healthy 86 year old, became ill soon after vaccination, first with diarrhea, then all of his organs began to shut down, and he died 18 days later.
He had no symptoms of Covid-19, but when they did an autopsy they found evidence of SARS-COV-2 proteins in all of his organs except his liver and olfactory bulb.
One of the many life-ending problems they found in his organs was Cardiac Amyloidosis.
The authors of the study certainly believed that the vaccination was the cause, even if Leung W-Y did not.
The third case this literature review looked at was presented at a conference, never written up as a study, and the abstract seems to have disappeared from the WHO website.
Another case of potential COVID-19 vaccination -induced amyloidosis describes a 60-year-old male of Laos descent who has been in Australia since the 1980s presenting with acute onset of peripheral edema and weight gain one week after receiving the second dose of mRNA Pfizer-BioNTech COVID-19 vaccine [64]. This case was not included in the final article list from our search given it was presented as a conference abstract at the 2022 Australia and New Zealand Society of Nephrology Meeting. The patient had no past medical history and was not taking regular medications, including over the counter remedies. Subsequent renal biopsy showed Congo red staining of amyloid deposits, and the bone marrow biopsy demonstrated 10% plasma cell aggregates via CD138 and amyloid deposit within the extramedullary tissue. At the time of this abstract’s publication, the patient had received bortezomib, cyclophosphamide and dexamethasone chemotherapy without hematological response and was awaiting work-up for a stem cell transplant.
Plausible Aetiology:
In Leung W-Y et al they outline some possible mechanisms for the aetiology of mRNA vaccine induced Cardiac Amyloidosis:
8. Proposed Pathophysiological Associations of COVID-19 Vaccination-Induced Amyloidosis
The paucity of reported cases describing COVID-19 vaccination-induced amyloidosis makes it challenging to decipher the pathophysiological associations which may explain this presentation. Nonetheless, raised SAA levels have been observed in other pathologies where there is COVID-19 vaccine-induced disease. One frequently discussed example is in COVID-19 vaccine-induced IgA disease (vasculitis and/or nephropathy), where marked SAA level increases were observed [65,66]. There are also other autoimmune conditions where SAA level elevations were noted [67]. The molecular mechanisms of how COVID-19 vaccination induces these disease manifestations remain largely unestablished. It has been postulated that the occurrence of these adverse effects appear as the result of acute inflammation caused by both the SARS-CoV-2 virus and the vaccine, given the symptomatic complications for many of these autoimmune conditions are similar in both viral-induced and vaccine-induced states [68,69]. The SARS-CoV-2 S protein, a common denominator between the virus and the vaccine, and soluble or endothelial cell membrane-attached angiotensin-converting enzyme 2 (ACE-2) is thought to play a significant role in the pathophysiological process, particularly if it enters the circulation and is systematically distributed around the human body [68,70,71]. More novel basic scientific evidence have suggested the potential of ionizable lipids within S protein mRNA-containing lipid nanoparticles to trigger pro-inflammatory responses following mRNA vaccination, by the activation of Toll-like receptors [72,73]. It has been found that lipid nanoparticles used in nucleoside-modified mRNA vaccine mice studies are highly inflammatory, evidenced by excessive neutrophil infiltration, activation of diverse inflammatory pathways, and production of various cytokines and chemokines [73]. This may have subsequently stimulated the processes of amyloid formation as described in the ‘proposed pathophysiological associations of COVID-19 induced amyloidosis’ section. Inflammatory responses via the lipid nanoparticles pathway are thought to be more severe in those with pre-existing inflammatory or autoimmune disease (e.g., if they have pre-existing amyloidosis) as demonstrated in a mouse model administration of mRNA–lipid nanoparticles, wherein this effect was shown to be specific to the lipid nanoparticle pathway only [74].
An even more plausible aetiology - Frame Shifting in mRNA vaccination causing amyloid proteins.
Since Leung W-Y et al literature review was published, however, another study, Mulroney et al, was published in December of 2023, and what this study reveals is that the mRNA vaccines are highly likely to cause misfolded proteins, also called Amyloid proteins.
Mulroney, T.E., Pöyry, T., Yam-Puc, J.C. et al.N1-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting. Nature (2023). https://doi.org/10.1038/s41586-023-06800-3
What is frame-shifting?
Frame-shifting in mRNA production is actually a disastrous outcome for what is supposed to be a life-saving medication.
Igor Chudov gives this excellent example of what frame-shifting means in a computer context:
For instance, computer characters comprising “GOOD MORNING” are encoded by the following bits:
What if a computer error deletes one bit in the second letter of “GOOD MORNING”?
The bits would shift and would encode a garbage sentence
“G^ЮИ@ЪЮдЬТЬП”
PROTEINS ENCODED IN THREES
Computer code uses 1s and 0s (called bits), and is usually encoded in bytes, or groups of 8 bits — but RNA is actually encoded in nucleobases, which can be uracil U), adenine (A), cytosine (C), and guanine (G). These are like the bits in computer code. RNA is encoded in sets of three nucleobases, which form codons, which are like the bytes, or individual letters, in the computer code.
caption...
In the mRNA vaccines, they substitituted an alternative nucleobase for Uracil, because the immune system could recognise Uracil in foreign mRNA and rejected it — so they used methyl-psuedo-uridine because it was invisible to the immune system, and could ‘slip under the radar,’ essentially, when the fake mRNA was uploaded to the cell nucleus to be replicated.
What the makers of the mRNA vaccines didn’t realise was that the methyl-psuedo-uridine was also invisible to the replication process in the cell.
Now, when one of the Uracils is skipped1, you get a completely different code:
What this code will produce is a completely different, unintended, protein; and it is highly likely that this protein will be one that cannot fold correctly.
In other words, frame-shifted genetic codes will result in random proteins, the vast majority of which will not be able to fold correctly, this is because the number of possible proteins that can fold correctly is actually vanishingly small (incidentally, this is actually a wonderful fact, that proves that life upon earth was surely designed and did not arise by chance, see my footnote2).
However, proteins that do not fold correctly are called amyloids, and amyloids are the cause of Cardiac Amyloidosis.
The frame shifted proteins outnumber the correctly translated ones by up to 900% in Pfizer BNT162b2
This little chart from Mulroney et al (Willis) is telling us that frame-shifted proteins in the mRNA vaccines outnumber the correctly translated proteins by up to 900%:
The mRNA vaccine does not stay at the injection site, but goes to the heart (and other organs)
Now we know from the TGA freedom of information release of the Pfizer Nonclinical Evaluation report3, that the lipid nanoparticles tend to go to the heart. In these rats, mRNA Lipid nanoparticles clearly went to the heart between 6 hours and 24 hours after vaccination.
Cardiac Amyloidosis
Now the question we are asking is, could Cardiac Amyloidosis that occurs after mRNA vaccination be caused by the mRNA vaccine?
(Particularly if myocarditis was seen in the patient immediately after vaccination, as in one of the studies cited above)
Temporality is the fourth item in the Bradford Hill criteria of causality; did this happen after vaccination but not before?
The name Cardiac Amyloidosis tells us everything we need to know: that this is a disease involving Amyloid Proteins; i.e. misfolded proteins.
But if Cardiac Amyloidosis occurs after mRNA vaccination, considering that mRNA frame shifting causing misfolded proteins is not only a distinct possibility but a large likelihood, could there be a connection between mRNA vaccination and Cardiac Amyloidosis?
To borrow Igor Chudov’s famous phrase, what do you think?
~~~~
Afterthoughts
Amyloid diseases
Misfolded proteins are actually associated with a large number of other diseases as well:
One thinks they should have thought of this possibility: presumably because Pseudo-uridine is not uracil, just as the immune system misses it when scanning for foreign mRNA, the mRNA translation process can’t seem to recognise it either.
In fact, mathematically speaking, Proteins that can fold correctly are extremely unlikely to have arisen by chance, and that these proteins are in abundance in the body is proof of intelligent design. https://www.discovery.org/m/2020/05/DNA-by-Design-Stephen-Meyer.pdf Stephen C. Meyer Dna By Design: An Inference To The Best Explanation For The Origin Of Biological Information p. 530 After looking at the likelihood of proteins arising by chance, Meyer looks at the ‘so-called “minimal complexity” required to sustain the simplest possible living organism’ He says it ‘suggests a lower bound of some 250 to 400 genes and their corresponding proteins. The nucleotide sequence space corresponding to such a system of proteins exceeds 4300000. The improbability corresponding to this measure of molecular complexity vastly exceeds the most conservative estimates of the so-called "universal probability bound" of 1 chance in 10150, the point at which appeals to chance become absurd given the "probabilistic resources" of the entire universe.’
South African scientist Etheresia Pretorius and her coworkers reported their magnificent paper from 2016 One Molecule of Endotoxin triggers clotting of 100,000,000 Fibrin molecules and that they are indeed Amyloid.










South African scientist Etheresia Pretorius and her coworkers reported their magnificent paper from 2016 One Molecule of Endotoxin triggers clotting of 100,000,000 Fibrin molecules and that they are indeed Amyloid.
https://geoffpain.substack.com/p/conformal-white-fibrin-clots-are