

Claim: Masks work to prevent spread of Covid
The study results fail to prove this.

There are some large studies into mask wearing to prevent Covid. The results do not prove to my satisfaction that wearing masks helps protect against the spread of Covid.
The Danish study in March 2021, the only study that tested masks against no masks, finds no statistically significant result between cloth masks and no masks. But in fact, there is significant suspicion that this study has been altered to make it publishable in the current politically correct academic world: according to the British Medical Journal their initial conclusion was that masks do not work.
The Vietnam study, a very rigorous study, finds no difference between cloth masks and surgical masks, and finds that all are leaky and ineffective at preventing Covid.
A preprint study in Finland found face masks did not impact Covid 19 spread among 10-12 year olds in Finland. This was a huge study comparing two cities and this was the result:
We compared the differences in trends of 14-day incidences between Helsinki and Turku among 10–12-year-olds, and for comparison, also among ages 7–9 and 30–49 by using joinpoint regression. According to our analysis, no additional effect seemed to be gained from this, based on comparisons between the cities and between the age groups of the unvaccinated children (10–12 years versus 7–9 years).
This is actually a much better study than the study in Bangladesh, because the two cities are highly comparable in population and other metrics, they are separate cities, and it does a direct comparison between masking and not masking.
The widely touted Bangladeshi study had 600 villages participating, 300 with an intervention encouraging people to wear masks, 300 with no intervention. The stated results are that mask wearing decreases Covid transmission by 10% - however the problem is that this study’s conclusions are weakened considerably by the fact that it is simply not a rigorous study comparing mask wearing to not wearing masks.
It is actually comparing an intervention encouraging people to wear masks, to no intervention, and when you do a study like this you are dealing with real people with contradictory and illogical behaviours in a context with many different unknown variables, so their conclusion is questionable for a number of reasons.
The study comes to the conclusion that there was around 30% extra mask wearing in the villages with the intervention (how do they know this? Did they watch every person in the village 24/7? This conclusion must be based on observation of a small percentage of the people a small percentage of the time, in which case you would have to question the confidence level) and they find that there was 9-11% less Covid in those villages in aggregate, which doesn’t seem like a large reduction! And this result is questionable, as there was a large enough percentage of participants who did not consent to blood tests in the villages with the intervention to cast the results into doubt, at least for cloth masks.
Additionally the study does not distinguish between the various possible effects of the intervention. It might not be masks at all causing that difference: it could be that people who were being constantly reminded and harassed to wear masks also remembered that they ought to stay home and isolate when they had symptoms. In which case it might be better to just tell them to do that. Or, having the possibility of catching Covid in mind constantly because of being reminded to wear masks, they may have tested themselves for Covid more often. One of the problems with the study according to James Lyons Weller is that they tested a lot of different subgroups, but didn’t do multiple hypothesis testing. What this means is that the likelihood of getting false positives is increased; one can easily cherry pick what one expects to find, which is something we tend to do quite unconsciously.
So I agree with what James Lyon-Weller says in the video below - the result appears somewhat unimpressive; I’m not sure it would all be worth it for a mere 10% reduction, and it certainly is not proven that this reduction was simply because more people were wearing masks:
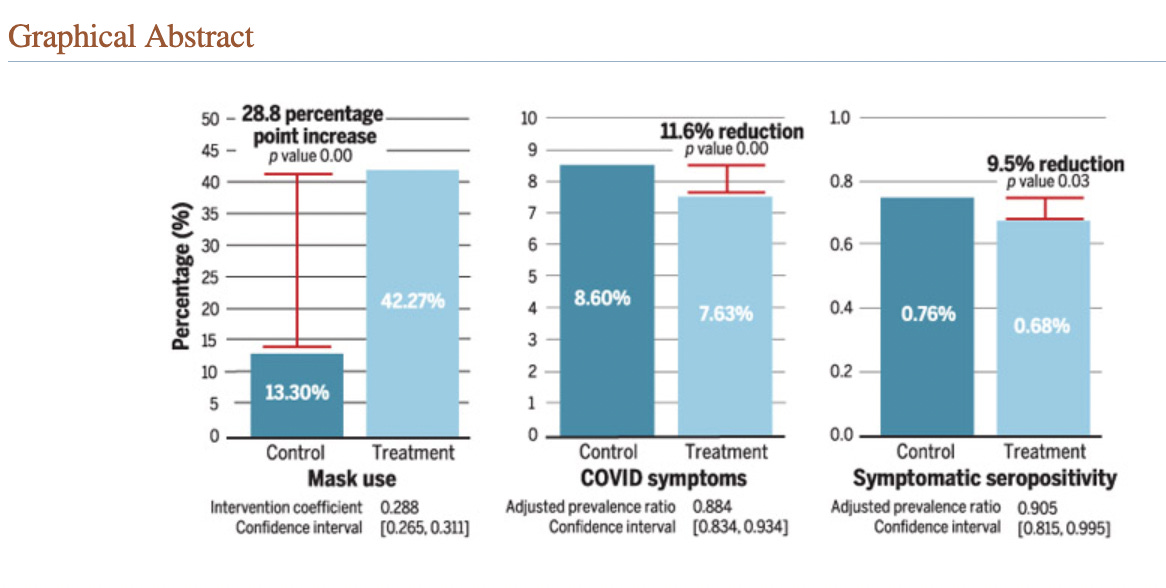
Indeed, despite the stated P value of 0.03, I’m really not convinced by a mere 10% reduction, particularly when it is clear that enough people in the villages where cloth masks were supplied did not consent to being tested for Covid that they had to impute missing values to get statistical significance for cloth masks; which essentially makes their result for cloth masks completely invalid. Imputing data is not proper science.
We found clear evidence that surgical masks are effective in reducing symptomatic seroprevalence of SARS-CoV-2. Although cloth masks clearly reduce symptoms, we find less clear evidence of their impact on symptomatic SARS-CoV-2 infections, with the statistical significance depending on whether we impute missing values for nonconsenting adults. The number of cloth mask villages (100) was half that for surgical masks (200), meaning that our results tend to be less precise. Additionally, we found evidence that surgical masks were no less likely to be adopted than cloth masks. Surgical masks have higher filtration efficiency, are cheaper, are consistently worn, and are better supported by our evidence as tools to reduce COVID-19 cases.
There are so many uncertainties in such a study: for instance, what if the intervention encouraging masks put 10% of people off getting tested for Covid if they had symptoms? What if more people stayed home when they were symptomatic? Ascribing the result to usage of masks in particular is overreach: this brings up that old nugget in statistics: Correlation is not Causation.
And a more significant reason that I doubt the results of the Bangladesh study is that there was also a much more rigorous study comparing cloth masks to surgical masks in a high risk hospital setting in Vietnam. There was found to be no difference between cloth masks and surgical masks; both were found to be very leaky and ineffective at preventing infection. A hospital is in effect almost a closed system: it is a far more scientific setting to test a hypothesis than a messy, real-life place such as a village where very little can be controlled, much less observed.
Also Mike Deskevich, a statistician looked at the raw data of the Bangladesh study on github and noticed this:

Good grief! The colour of the mask makes a difference??? This does not make any sense. It’s very clear that there is a lot of noise in this study.
Further discussion of this in the addendum.
https://rumble.com/v11453u-interview-with-mike-deskevich-on-the-bangladesh-mask-study.html
This UBS debate with Jason Abaluck, the principal author of the Bangladeshi study, is quite long; however the important discussion begins at about 46 minutes. See what you think of his answers to James Lyon-Weller’s objections.
References
Abaluck J, Kwong LH, Styczynski A, Haque A, Kabir MA, Bates-Jefferys E, Crawford E, Benjamin-Chung J, Raihan S, Rahman S, Benhachmi S, Bintee NZ, Winch PJ, Hossain M, Reza HM, Jaber AA, Momen SG, Rahman A, Banti FL, Huq TS, Luby SP, Mobarak AM. Impact of community masking on COVID-19: A cluster-randomized trial in Bangladesh. Science. 2022 Jan 14;375(6577):eabi9069. doi: 10.1126/science.abi9069. Epub 2022 Jan 14. PMID: 34855513; PMCID: PMC9036942. https://pubmed.ncbi.nlm.nih.gov/34855513/
Bundgaard H and Bundgaard J S, et al. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers Annals of Internal Medicine March 2021 https://doi.org/10.7326/M20-6817
MacIntyre CR, Seale H, Dung TC, Hien NT, Nga PT, Chughtai AA, Rahman B, Dwyer DE, Wang Q. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015 Apr 22;5(4):e006577. doi: 10.1136/bmjopen-2014-006577. PMID: 25903751; PMCID: PMC4420971. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4420971/
Juutinen A, Sarvikivi E, Laukkanen-Nevala P, Helve O. Use of face masks did not impact COVID-19 incidence among 10–12-year-olds in Finland doi: https://doi.org/10.1101/2022.04.04.22272833
https://stevekirsch.substack.com/p/masks-fail-their-latest-test?s=w
BMJ article about the study from Denmark. https://www.bmj.com/content/371/bmj.m4586
Addendum - Discussion between Mike Deskevich and Steve Kirsch.
A summary of this discussion:
https://rumble.com/v11453u-interview-with-mike-deskevich-on-the-bangladesh-mask-study.html
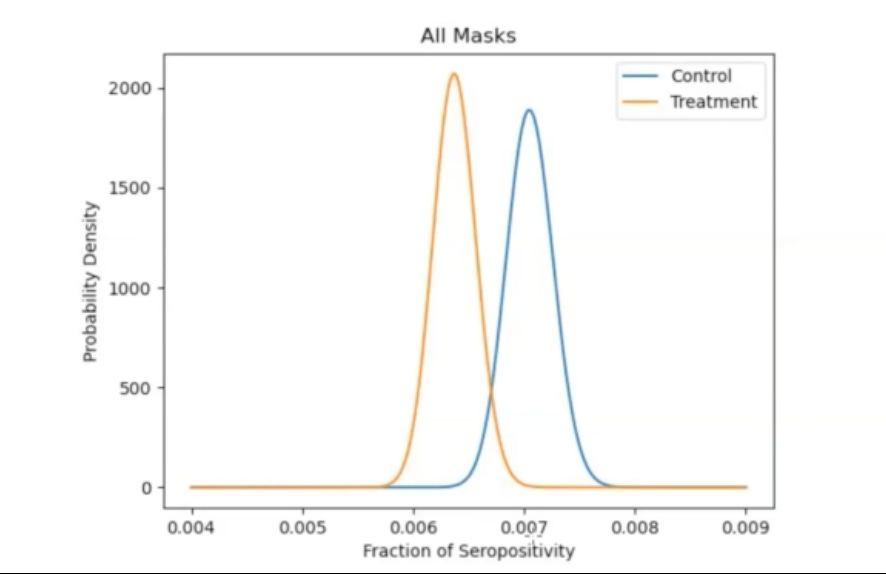
Mike Deskevich, a statistician looked at the raw data on github and was not convinced; the uncertainty in the measurement is so large you can’t make any clear statement. Apparently the Bangladeshi calculated the p value based on individuals, but they probably should have calculated the p value based on villages. Also they tested for prior Covid infections after randomisation, which they should have done before randomisation (what if some villages had had a prior Covid wave?)
This chart means the difference between all masks and no masks means the difference is about 1 person less in 1000 catching Covid.
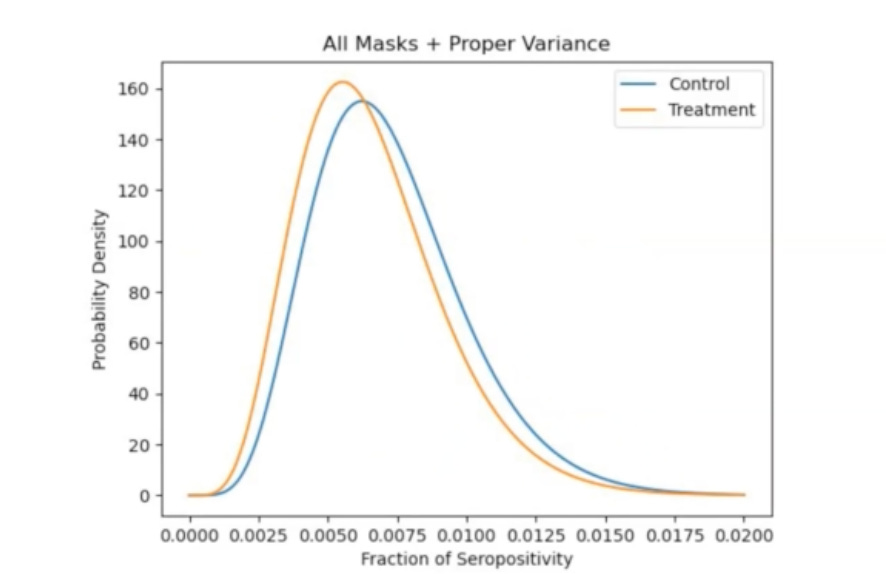
This chart shows the P value with sample size per village, the area where the curves overlap is the P value, greater than 0.05.

Furthermore they didn’t test all the people with symptoms, only about 10,000 people. Taking into account that fact Deskevich comes up with this curve:
He makes the point that the study does not show that masks work; the following graphs show that the control groups are inconsistent - this is a real problem actually…! It’s really bad. How can the control group for cloth masks be different than the control group for surgical masks??? (First Fact Check note - is this in the data, or something in the way Mike Deskevich graphed the data?)
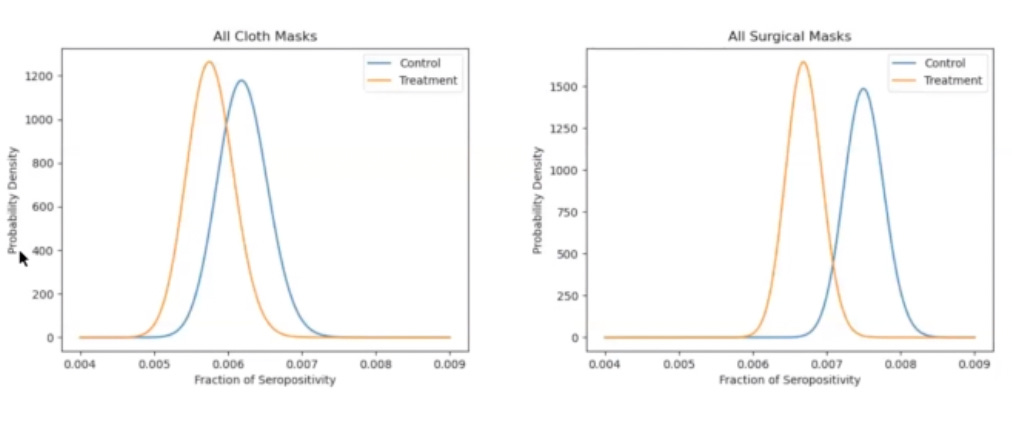
Good grief! The colour of the mask makes a difference??? This does not make any sense.
It’s very clear that there is a lot of noise in this study.
I would certainly like to see by Jason Abaluck do a proper rebuttal of Mike Deskevich’s points, if I am to believe that masks make any difference to Covid infections.
https://rumble.com/v11453u-interview-with-mike-deskevich-on-the-bangladesh-mask-study.html
Change log
Added the addendum and the red mask purple mask chart.